 |  |  |
| T2 | FIR | T2 1 year later |
| | | |
| T2 | FIR | T2 1 year later |
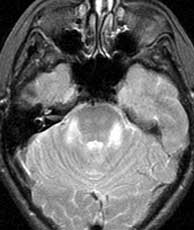
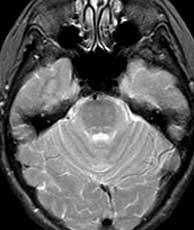
The differential for this appearance, particularly given the follow-up exam showing interval improvement, is limited. Central pontine myelinolysis may produce transient increased T2 signal within the pons and is believed to occur secondary to rapid correction of low serum sodium. Most of the abnormal signal in this case; however, is in the middle cerebellar peduncles. Furthermore, the clinical history does not match. Rhombencephalitis is a rare inflammation of the brainstem, which has been reported in relation to the listeria among others. This disease produces foci of increased T2 signal within the brainstem thought to be ischemia due to vasculitis. Neoplasm is not in the differential secondary to the bilateral symmetric appearance as well as the interval partial resolution. One might consider infarct on the first study in the right clinical setting; however, the bilateral asymmetry of the signal abnormality weighs heavily against that diagnosis. Related Cases
Tokonami F, Imamura S, Suga M, Tokunaga K, Fukuda Y. A case of Listeria rhombencepalitis with a secondary vascultis suggested by MRI. Rinsho Shinkeigaku, Jun 1993; 33(6):p637-41.
Korogi Y, Takahashi M, Shinzato J, Sakamoto Y, Mitsuzaki K, Hirai T, Yoshizumi K. MR findings in two presumed cases of mild central pontine myelinolysis. AJNR, May-Jun 1993; 14(3):p651-4.
 |  |  |
| Hypertrophic olivary degeneration | Brainstem glioma | Pontine infarct |