 |  |  |
| T1 pre-gad | T2 | T1 pre-gad |
| | | |
| T1 pre-gad | T2 | T1 pre-gad |
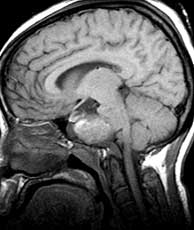
The differential in this case is complicated by the fact that there are two lesions. Other entities to consider when faced with a large mass which seems to involve the clivus primarily are chordoma and chondrosarcoma although these tend to be off midline where chordomas are in the midline. Other skull base lesions more commonly seen in older patients may include metastases and plasmacytoma. Occasionally craniopharyngiomas attain a huge size obscuring their true origin. In this case, the diagnosis of bilateral cholesterol granulomas is not listed in the differential because of its extreme rarity. It maybe considered in retrospect, however, if you notice that the lesions seem to be centered in each petrous apex and appear to kiss in the middle. This is best appreciated on the coronals. Related Cases
Henick DH, Feghali JG. Bilateral cholesterol granuloma: an unusual presentation as an intradural mass. Journal of Otolaryngology, Feb 1994; 23(1):p15-8.
Thedinger BA, Nadol JB Jr, Montgomery WW, et al. Radiographic diagnosis, surgical treatment, and long-term follow-up of cholesterol granulomas of the petrous apex. Laryngoscope, Sep 1989; 99(9):p896-907.
Smith PG, Leonetti JP, Kletzker GR. Differential clinical and radiographic features of cholesterol granulomas and cholesteatomas of the petrous apex. Ann Otol Rhinol Laryngol, Nov-Dec 1989; 97(6 Pt 1):p599-604.
Greenberg JJ, Oot RF, Wismer GL, et al. Cholesterol granuloma of the petrous apex: MR and CT evaluation. AJNR, Nov-Dec 1988; 9(6):p1205-14.
Gamache FW Jr, McLure T, Deck M, et al. Bilateral cholesterol granuloma of the skull base: case report and review of the literature. Neurosurgery, Jun 1988; 22(6 Pt 1):p1098- 101.
Griffin C, De La Paz R, Enzmann D. MR and CT correlation of cholesterol cysts of the petrous bone. AJNR, Sep-Oct 1987; 8(5):p825-9.
 |  |  |
| Chordoma | Craniopharyngioma | Cholesterol granulomas |